
HIMS: The Tough 'Ask' for Filling the GLP-1 Void
The critical visual to understand the GLP-1 'cost' in a post-shortage world

Disclaimer: All information provided herein by Cedar Grove Capital Management, LLC (“Cedar Grove Capital” or “the fund”) is for informational purposes only and does not constitute investment advice or an offer or solicitation to buy or sell an interest in a private fund or any other security. An offer or solicitation of an investment in a private fund will only be made to accredited investors pursuant to a private placement memorandum and associated documents.
Cedar Grove Capital may change its views about or its investment positions in any of the securities mentioned in this document at any time, for any reason or no reason.
Students can get access to our research at a reduced rate by clicking here. If you’re interested in using Koyfin (I highly recommend it), you can get 20% off your plan using my link here.
Interested in becoming an LP? Click here to fill out the contact form.
The Need for ‘Keeping Pace’
We posted about this in our report the other week (below) but we’ve made a visual for those interested who have yet to do the math.

The above report is a shorter follow up to what was our longer report (20-pages) after Q4’24 earnings (below).

Looking at all of our GLP-1 options for Weight Loss in a post-shortage world, the math needed to make up for the lost earnings speaks for itself.
Referring to the image below, HIMS can no longer sell commercially available Compounded Semaglutide unless it's personalized and only if the patient has an absolute need for one.
But the point of this visual is to highlight what expectations are needed in order to drum up the same level of business that HIMS was experiencing during their loophole exploitation.
Let's start off with the basics.
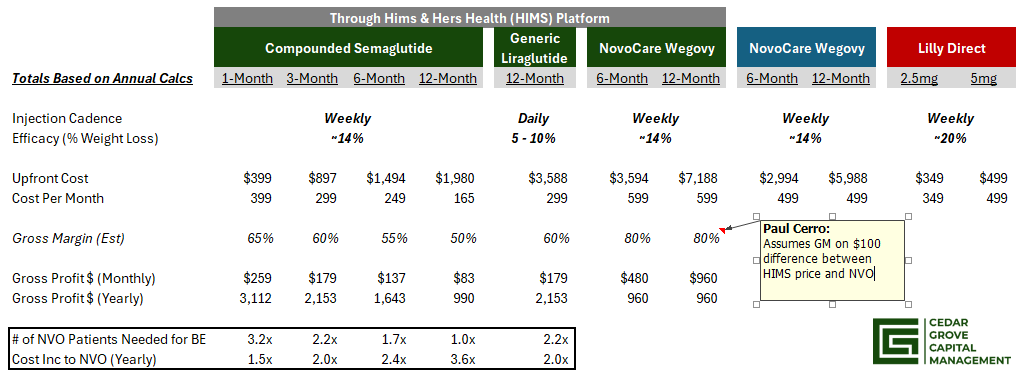
Looking at the chart, we've outlined the various prices that HIMS was offering subscribers dependent on their ordering cadence (1, 3, 6, or 12 months).
For generic Liraglutide, the cheapest option is only advertised as a 12-month upfront payment. Novo’s Wegovy, through HIMS, is listed at $599/month but requires a 6-month upfront payment.
Our gross margins are assumptions and seem to track given how quickly HIMS gross margin was falling since the end of Q3.
Results:
Compounded Substitution
In order to get the same level of gross profit from the new NovoCare partnership as opposed to the compounded Semaglutide option, you would need anywhere from 1 - 3.2 incremental NovoCare subs to get that.
However, you would also be asking them to pay anywhere from 1.5x - 3.6x MORE than they were just paying in order to get it.
Conversely...
Generic Liraglutide
If you were banking on Generic Liraglutide to save the day, think again.
If our estimates are correct, you would need ~2.2 NovoCare subs in order to get the same GP while also asking them to pay 2x more than they otherwise would have.
Other Considerations
Generic Liraglutide is a daily injection (worse retention) and also leads to less weight loss (less efficacious) - we've talked about this is past reports.
Wegovy is a weekly injection but shows patients, on average, lose ~14% of their weight.
NovoCare is offering Wegovy at $100 cheaper on their own site rather than going to $HIMS
LillyDirect offers their Zepbound starting at $349/mo, which is 30% cheaper than getting it directly on NovoCare or ~42% cheaper than using HIMS for a more efficacious drug (~20% weigh loss)
So when comparing the options, you need to consider two things.
In order to make the same level of gross profit, you're asking more subscribers to shell out more money because of how the dynamics have changed.
If price is the deciding factor, why would subscribers go to HIMS when they can get Wegovy much cheaper directly on NovoCare? Or if they wanted the superior weight loss drug (Zepbound), why wouldn't they just go to LillyDirect where not only is it cheaper but it is more efficacious?
To reach the $725 million in weight loss for FY'25, you're really asking $HIMS to be able to entice enough subscribers to sign up for 1 of their many options that are either way more expensive for arguably the same or worse weight loss, or less expensive options (orals) which also are less efficacious.
Hope this helps anyone who hasn't looked at it this way yet.
As always, we appreciate your support of our work. If you have any questions, please make sure to message or comment below. If you think others would benefit from the research/commentary we release, we would greatly appreciate your sharing.
Until next time,
Paul Cerro | Cedar Grove Capital
Personal Twitter: @paulcerro
Fund Twitter: @cedargrovecm